Aged Care in Australia 2007 – 2008
The Minister for Ageing, Justine Elliot, commented in her media release in November, 2008:
- During 2007-08, the Aged Care Standards and Accreditation Agency conducted 5,244 visits to aged-care homes. 3,105 visits were unannounced.
- In this same period the Department of Health and Ageing undertook 3,127 visits to aged-care homes, of which 1,145 were unannounced.
- The Accreditation Agency identified 46 homes (1.6 per cent) that had some non-compliance in relation to the 44 accreditation standard outcomes.
--- The Minister made further comment in her media release on 26 November, 2008:
"The data speaks for itself. It shows the vast majority of nursing homes are providing a world class service, but there is a small group - 46 nursing homes - that had failed to meet 44 accreditation standard outcomes under the Aged Care Act."
When 46 failed homes really means 199
The Minister also states in the Report on the Operation of the Aged Care Act 1997 - 1 July 2007 to 30 June 2008:
"only 1.6 per cent of homes (46 homes) were identified as having some non-compliance in respect to the 44 Accreditation Standard expected outcomes"
Aged Care Crisis records indicated that at least 108 (3.8%) of aged-care homes did so. We wrote to the Minister prior to publishing our findings along with supporting data, seeking clarification of the discrepencies, together with the data source available to us at the time.
This was based on information that we were able to access published on-line (at various stages throughout the year) by the Agency and the Department. Based on the limited information that is publicly available, the data may not be contemporaneous and these findings were tentative at the time.
Update - 16 Dec 2008: After being approached by media, The Minister stated that 199 (7%) of aged-care homes were identified as having some non-compliance over the year.
Update - 16 Jan 2009: A reply from the Minister's office, along with an explanation of the number of non-compliant nursing homes figures from 46 Vs. 199:
"The Report correctly indicates that, on 30 June 2008, 46 aged care facilities were operating with some level of non-compliance with the Accreditation Standards. The Report does not include instances of non-compliance in cases where the non-compliance was rectified prior to 30 June 2008."
* "I appreciate that this may not be clear to readers and we will review how the figure is represented in future reports."
* Groundhog day: Fast forward to 2016, and the renamed Quality Agency seem to have adopted the same style of reporting.
Analysis
Distribution of aged-care homes
As of June 30, there were 2,838 Commonwealth-funded aged-care homes in Australia. The proportion of aged-care homes, expressed as a percentage figure, is shown in Figure 1 (below).
The Minister's report and other data available to us indicate that not-for-profit groups operated 1,698 (59.7%) homes. Of these 821 (29%) were run by religious groups, 481 (17%) by charities, and 396 (14%) by community based groups.
Governments operated 198 (7%) and private-for-profit operators 942 (33.7%). This categorisation is based on a document which we believe originated within the Department of Health and Ageing.
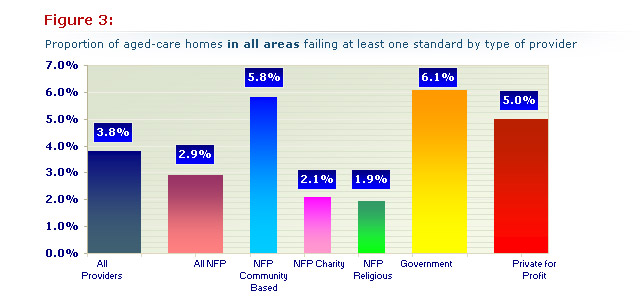
Distribution of aged-care homes not meeting at least one required standard
The distribution changes when the 108facilities that failed at least one accreditation standard are examined. Private-for-profit 47 (44%), government 12 (11%) and community-based not-for-profit 23 (21%) each had an increased proportion of the failed homes. In contrast, charitable 10 (9%) and religious not- for-profit 16 (15%) had a much smaller proportion. They accounted for only a quarter of the failed aged-care homes even though they operate nearly half of all aged-care homes (Figure 2)
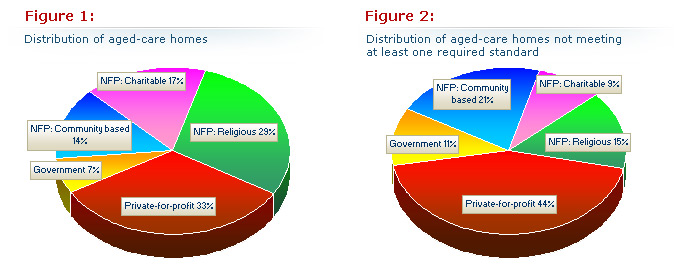
In Figure 1 (left), the proportion of all 2,838 Australian nursing homes by approved provider type (left) compared with Figure 2 (right) the proportion of 108 Australian nursing homes that had some non-compliance by approved provider type. Note that the charitable and religious groups have halved the proportion of the failed homes whereas the other three have increased indicating that the problem homes lie mainly here.
Incidence of failures
Using the figures above it was possible to calculate the proportion of aged-care homes failing an accreditation standard in each group and then compare the rate of accreditation failures for each to give an indication of performance in Figure 3 (below):
The best performers were the charitable and religious not-for profit sub-groups. They had less than half the rate of private-for-profit providers and almost one third the rate of government-run and community-based not-for-profit aged-care homes.
A more accurate, but still not fully comparable comparison between the private-for-profit and not-for-profit providers, is given by comparing the for-profit private providers with the charitable and religious not-for-profit groups only. The latter operate fewer peripherally located failing services (23%) than the government and community based groups (63%). Only 4% of the failing private-for-profit providers are peripheral with 96% central. When compared with the charity and religious groups, the private-for-profit operators had more than double the proportion of failing homes - see Figure 3 (above).
Number of standards failed
The average number of the 44 accreditation standards failed did not differ much between the various groups. The charitable and not-for-profit religious organisations had fewer but the numbers were insufficient to draw any firm conclusions.
Government operated aged-care homes averaged 10.7 failures, community-based not-for-profit 9.7, not-for-profit charitable 6.0, not-for-profit religious 6.9 and private-for-profit 9.0.
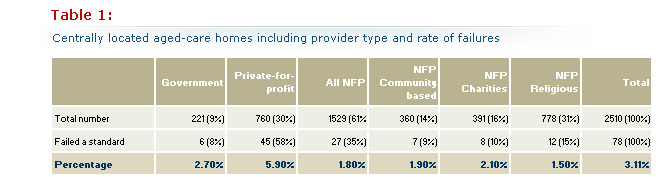
The impact of distance
Isolation by distance from major centres and medical services is likely to be associated with limited management resources, fewer trained staff, and less oversight by parent organisations and other bodies. They are therefore at a disadvantage.
The differences in distribution between peripheral groups of aged-care homes in outer regional, remote and very remote areas - when contrasted with central groups comprising inner regional and major city areas - is striking. These readily account for the differences seen between the government and community-based groups on the one hand and the charitable and religious groups on the other. Both are more likely to serve those in need in their own localities.
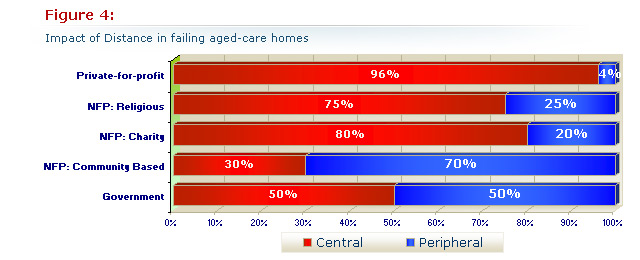
Figure 4 (above), shows the proportion of the 108 nursing homes failing at least one standard owned by each sort of provider group in central and peripheral areas.
The impact of private-for-profit control of aged care
As a more peripheral location clearly was associated with failures in standards we re-examined the data after excluding all of the peripheral facilities. To get the information we needed we used a different data source with 2,937 (107 more facilities) listed in Australia. This was not a significant difference, We excluded 427 peripherally located facilities leaving 2,510 more central ones for analysis. When we excluded the 30 peripherally located aged-care homes that had failed a standard we were left with 78 that were centrally located. The distribution of both groups by provider group as well as the rate of failure is shown in Table 1 (below):
The percentages of failed aged-care homes graphed in Figure 5 (below) can be compared with Figure 3. The bias created by distribution has disappeared so that government and not-for-profit subgroups now perform similarly.
The private-for-profit sector stands out with more than twice the incidence when compared with government, over three times when compared with all not for profits and almost four times when compared with the largest not-for-profit group, the religious providers.
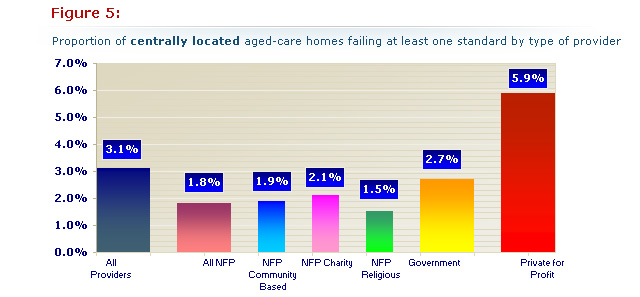
Figure 5 (above): Note that the change in distribution in each group differs from our first analysis (Figure 3), in that the private-for-profit sector has more than double the rate of failing aged-care homes than all the other groups which now perform comparably.
Additional comments and information
The following sliders contain additional information and comments about the data and the accreditation process:
